I'm not sure where to start this update. On one hand, a lot is happening, but on the other hand, not much is happening. I had my most recent monthly visit on June 6. As with the previous visits, all the tests came out negative, including the urine test.
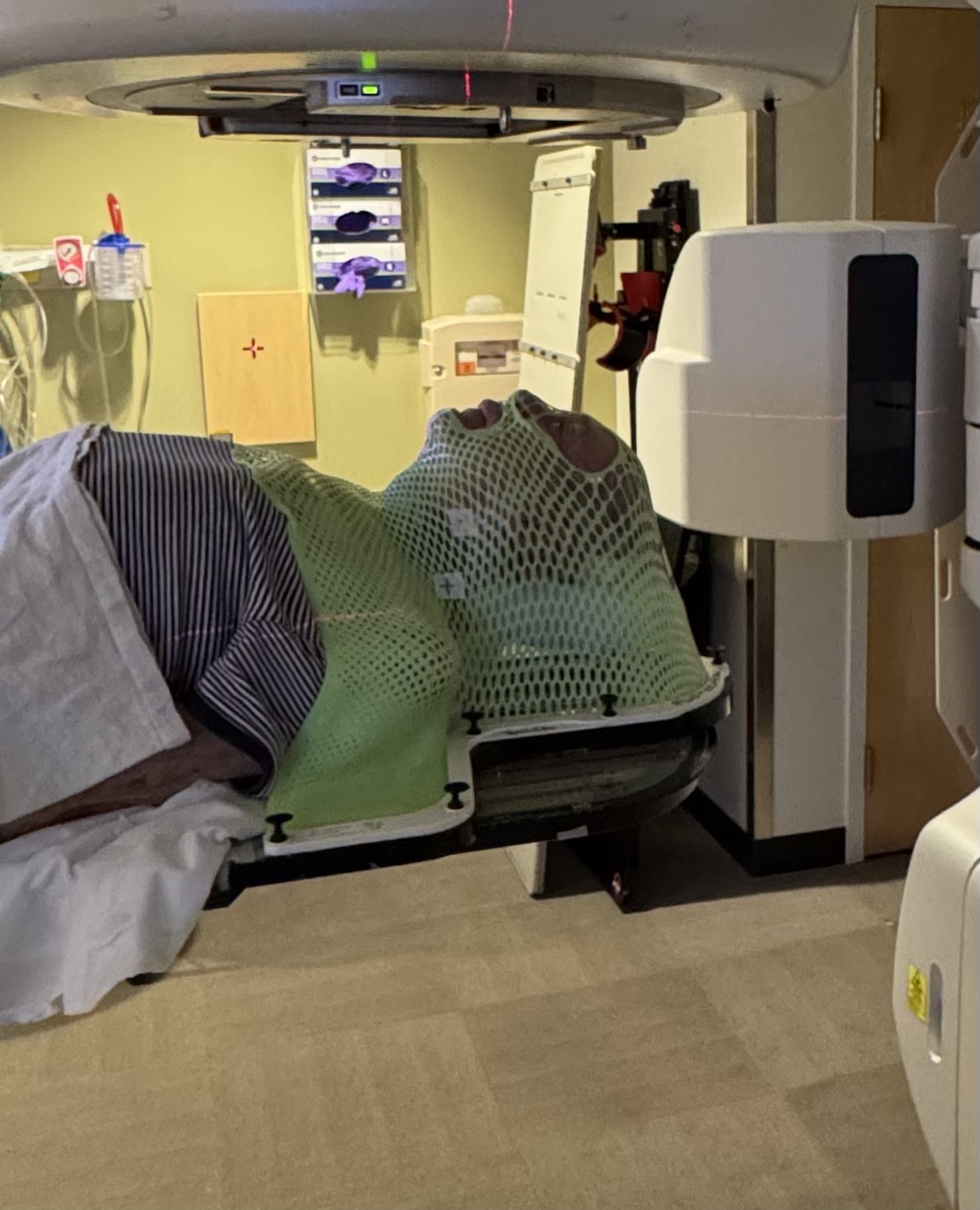
I'm a little confused by that, as it happens that the nodule in my cervical spine seems to be MM. How can that happen? Dr. Richardson prescribed radiation treatment, which I have undergone. I had 5 sessions of stereotactic body radiation therapy (SBRT) focused on this lesion. Here is a picture of the hard plastic mask they used on me for the treatments:
In the meantime, I had a visit with Dr. Richardson on June 16. He was concerned about the nodule in my left neck. It seems that it may be associated with the scalp skin cancer I've been dealing with. He thinks it might be an infection, so he prescribed a 10-day course of antibiotics (Cephalexin, 2,000mg/day), along with mouth hygiene. I've finished that.
Two of the three squamous cell carcinomas on my scalp have been surgically removed over the last couple of weeks, and I'm recovering from those. The third one is scheduled for August. I hope these surgeries will help with this infection, if that's what it is. Another possibility is that it is a metastasis of the skin cancer to the lymph node in my neck. I hope not!
I have my next regular visit to Dana-Farber on July 7. However, I don't have any tests scheduled to determine whether any of the therapies I'm going through are working. No MRI, no biopsy, no nothing. So, how can I find out where I stand with all of this? It's a bit confusing.
Dr. Richardson wants me to continue with the clinical trial I'm on for now, but he plans to change that in the future, depending on how the antibiotic treatment works. He wants me to go on anti-B-cell maturation antigen (BCMA) therapy. There are two types of anti-BCMA therapies available.
The first is CAR-T cell therapy, wherein T-cells are extracted from the body and modified in the lab to attack cancer cells. The modified T-cells are then injected back into the body to do their work. The problem with this therapy is that it requires a hospital stay followed by extensive at-home health care. I don't know if I would qualify for this intensive treatment.
The other option is bi-specific T-cell engagers. These antibodies can attach directly to the cancer cell, as well as the immune system T-cell, thus bringing the T-cell into contact with the cancer cell to kill it. There are several of these engagers available that seem to be promising and are undergoing clinical trials.
I'm sure Dr. Richardson knows what he is doing and will prescribe the most efficacious treatment for me.
In the meantime, I'll just cross my fingers and hope for the best.








{kind=link}
{kind=link}
{kind=link}
{kind=link}